If I ask you, what’s the most beautiful and joyful time in a couple’s life? You might say,
Engagement or honeymoon, right?
You are wrong!
It is a pregnancy.
When a female partner says, “It’s positive.”
Suddenly, everything changes for them. But for some couples, this time, ‘every time’ comes up with anxiety, tension and nervousness. And that’s because of one condition that happens twice, thrice or during almost every pregnancy, the pregnancy loss or miscarriage.
In this case study, we will discuss the curious case of Recurrent Pregnancy Loss (RPL) in couples. And try to get some insights and novel outcomes.
We will discuss the case, gather key clinical and genetic information, explore the underlying genetics, and identify the major learning outcomes.
Previous case study: [Case Study #1] Why Did This Family Keep Dying at 8:00 AM?
Key Topics:
Key clinical information:
As per the WHO, two or more pregnancy losses have been considered as Recurrent Pregnancy Loss; however, some guides suggest 3 or more.
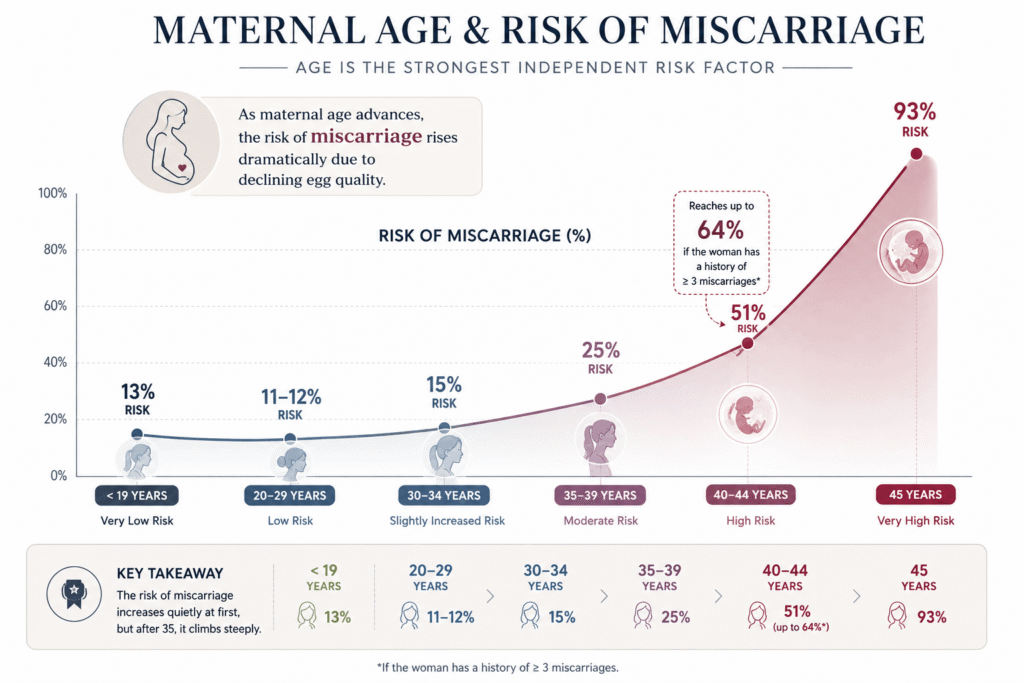
Put simply, when miscarriage or pregnancy loss happens multiple times, it is categorised as RPL. Factors causing this condition are maternal age, uterine deformities, genetics, thrombophilia, endocrine and immune disorders, infection and Lifestyle.
Among these, genetic factors are significant and notably prevalent with 50% frequency of chromosomal abnormalities either in both/any parent or in the fetus. In addition, trisomies, disomies, monosomies and single gene defects are also reported in the fetus.
Talking about the structural chromosomal abnormalities, one of the largest groups of abnormalities that cause RPL are balanced translocation, reciprocal and robertsonian translocation and inversions.
Interestingly, parental balance translocation is one of the most common genetic factors in RPL, found in 2 to 5% of couples.
In this case, the condition doesn’t cause any symptoms or abnormalities in either parent, but when it is inherited, it produces lethal fetal abnormalities and leads to RPL.
Patient Summary:
Zarifian et al. (2012) reported a case of parental balanced translocation in the RPL. The couple had a consanguineous marriage and are blood relatives. The ages of the male and female are 35 and 27, respectively.
The couple had four consecutive intrauterine fetal deaths. Their hormonal and uterine anatomical profiles are normal. However, the cytological investigations show a unique and interesting condition of balanced translocation in both.
Without revealing much information, the study showed no signs of underlying maternal disease or infection that can cause RPL.
What genetics reveal?
The high-resolution G-banding showed balanced translocation in both partners, a rare and unique situation. The female karyotype is 46, XX, t(16;6)(p12;q26). The balanced translocation occurred between the p12 band of chromosome 16 and the q26 band of chromosome 6.
Meaning, no gain or loss reported in the couple, which makes them absolutely normal without any physical abnormalities.
While no other chromosomal abnormalities have been reported, molecular investigation hasn’t been conducted.
Key observations:
Couples with balanced translocations produced abnormal gametes with imbalanced translocations. In this case, although the couple is phenotypically normal, the balanced translocation produces 25% of gametes being normal or balanced, while the remaining 75% are either unbalanced or otherwise chromosomally abnormal.
This results in either a missing or an extra part of either chromosome 6 or 16, resulting in aneuploidy and serious developmental problems in the fetus. This causes fetal death.
One of the interesting observations of this case study is that fetal death occurs before the 16th week of pregnancy.
Key learnings:
This case highlights the significance of genetic factors during pregnancy. Key learnings are listed here:
- Consanguineous marriages increase the risk of rare genetic overlap and they can transmit lethal genetic mutations to other family members.
- When both partners carry the same genetic abnormality, the fetal survival chances dramatically reduce.
- Genetic counseling and early testing help couples and doctors understand the exact cause of miscarriage most effectively.
Join Now!
Join our Karyotype Analysis Cohort and gain hands-on experience in chromosome analysis, karyogram preparation, ISCN nomenclature, and real clinical case interpretation. Learn from experts, strengthen your cytogenetics skills, and build confidence in reporting chromosomal abnormalities.
Enroll now and take the next step in your cytogenetics journey
Wrapping up:
Cytogenetic investigation remains one of the most important and valuable approaches for evaluating recurrent pregnancy loss (RPL) because of the high prevalence of numerical and structural chromosomal abnormalities.
However, advanced high-resolution techniques, such as FISH, chromosomal microarray analysis, and next-generation sequencing (NGS), have recently emerged as powerful complementary tools for genetic evaluation.
RPL isn’t an inherited condition, nor does it solely occur due to chromosomal abnormalities. Couples should undergo genetic counseling or take a doctor’s advice for better management and treatment.
Prenatal and pre-implantation genetic testing, and family screening can significantly lower RPL risks.
If you want to learn karyotyping and chromosomal investigation, you can join our karyotyping course. Click the link given above and join the class.
Reference: Zarifian, Ahmadreza et al. “Balanced chromosomal rearrangement in recurrent spontaneous abortions: a case report.” International journal of molecular and cellular medicine vol. 1,4 (2012): 225-8.