Imagine this…
A pregnant woman undergoes her routine first-trimester ultrasound.
Everything else looks normal, but the scan reveals several subtle developmental abnormalities. The obstetrician prescribed chorionic villus sampling (CVS) to investigate the baby’s chromosomes.
The chromosomal investigation looks completely normal.
The parents are relieved.
But the doctor wasn’t convinced and he recommended another genetic test instead of reassuring the couple.
Why?
If the CVS results are normal, shouldn’t the fetus also be normal?
Could the first genetic test be wrong?
Not exactly.
Sometimes the placenta and fetus do not share the same genetic makeup.
In our previous case study, we learned about Confined Placental Mosaicism (CPM), where the placenta is abnormal, but the fetus is normal.
This case is exactly the opposite.
The placenta appears genetically normal, while the fetus carries a complete chromosomal abnormality.
Let’s understand how this happened through a real clinical case.
Key Topics:
Key Clinical Information
A 28-year-old woman underwent a routine first-trimester ultrasound at 13 weeks and 2 days of gestation during her first pregnancy.
The scan showed a markedly increased nuchal translucency (NT) of 5.5 mm and reversal of the a-wave in the ductus venosus. This suggests an increased risk of fetal chromosomal abnormalities.
A follow-up ultrasound at 10 weeks showed even worse findings, including a large cystic hygroma, coronary sinus dilatation, and a persistent left superior vena cava.
The initial placental genetic testing demonstrated a normal karyotype, but the progressive ultrasound abnormalities strongly suggested that something was wrong with the fetus.
Patient Summary
The patient was a 28-year-old primigravida (G1P0). She doesn’t have any significant medical history of recurrent pregnancy loss, infertility or genetic abnormalities.
The fetal ultrasound results reveal
- nuchal translucency (NT) of 5.5 mm
- Reversal of the a-wave in the ductus venosus
- Nuchal cystic hygroma
- Coronary sinus dilatation, and
- Persistent left superior vena cava
Genetic Investigation
The first genetic investigation was performed using chorionic villus sampling (CVS) at 13 weeks and 2 days.
The placental sample was analyzed using:
- Chromosomal Microarray Analysis (CMA)
- Quantitative Fluorescent PCR (QF-PCR)
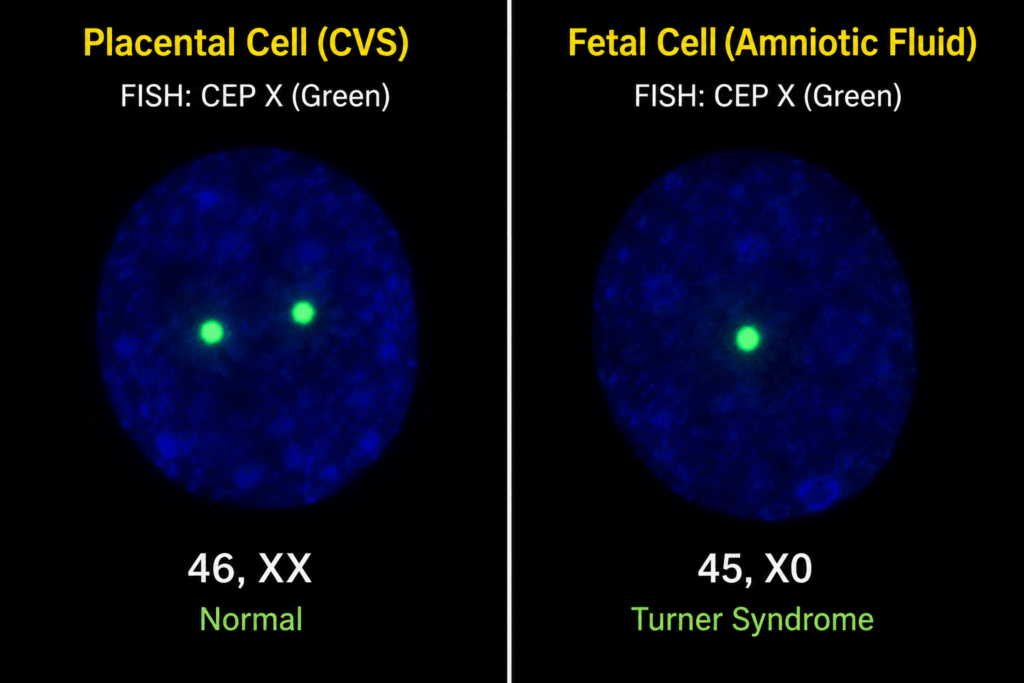
- Fluorescence In Situ Hybridization (FISH)
While both FQ-PCR and FISH showed an almost normal female karyotype, the CMA results indicated a low level of mosaic monosomy X. Initial findings indicated that the placenta was largely unaffected and did not have any chromosomal abnormality.
Amniocentesis was performed at 20 weeks as the fetal ultrasound abnormalities continued to worsen. The amniotic fluid was analyzed using the same three genetic techniques.
Unlike the placental results, all three investigations confirmed complete Monosomy X (45,X) in the fetal cells.
Following pregnancy termination, multiple tissue samples were collected from the placenta, amniotic sac, umbilical cord, fetal skin, and skeletal muscle.
FISH analysis demonstrated a remarkable genetic gradient.
The placenta contained very few monosomy X cells (0-6%), the amniotic sac showed moderate mosaicism (16-29%), while the fetal tissues showed almost complete monosomy X (88-98%).
Genetics Explained
This case represents an unusual form of fetus-confined mosaicism, which is essentially the reverse of Confined Placental Mosaicism (CPM).
During early embryonic development, the fertilized egg repeatedly divides before separating into two major cell populations.
The outer cell layer (trophectoderm) develops into the placenta, while the inner cell mass develops into the fetus.
If a chromosomal error occurs after these two cell lineages have separated, only one lineage may be affected.
In our previous CPM case, the chromosomal abnormality remained confined to the placenta while the fetus developed normally.
In this case, however, the opposite happened.
A mitotic error occurred in the cells destined to become the fetus, while the placental cells remained genetically normal.
As a result, CVS, which has been performed on the placental tissues, could not show any chromosomal abnormality.
Further molecular analysis confirmed that the placental X chromosomes originated from both the mother and the father.
This ruled out a meiotic nondisjunction followed by chromosomal rescue and demonstrated that the abnormality arose during early mitotic cell division in the developing embryo.
Related article: [Infographics]: Pregnancy Genetic Testing Guide.
Key Outcomes
This case demonstrates that a normal CVS result does not always guarantee a genetically normal fetus.
Although the placental cells appeared largely normal, the fetal tissues showed almost complete Monosomy X (45,X).
The progressive ultrasound abnormalities correctly indicated that additional investigations were necessary.
Key Learnings
Genetic testing and ultrasound observations are both needed to correctly locate if the abnormality is affecting the fetus or not.
CVS analyzes placental tissue, not fetal tissue directly.
Ultrasound results should always be considered the primary evidence for the fetal abnormality.
A well-structured screening and testing SOP is required for the detection of fetal abnormalities.
No single prenatal test is perfect. Doctors should always prescribe a confirmation test.
Wrapping Up
While Confined Placental Mosaicism teaches us that an abnormal placenta doesn’t always mean an abnormal fetus, this case study teaches us the complete opposite: the normal placenta doesn’t always mean a normal fetus.
And this also shows us that prenatal screening is much more complex than we think. A genetic counselor’s advice is always needed before making any pregnancy-related decision.
Clinical findings, laboratory testing and genetic investigations are required to strengthen prenatal decision-making.
Reference:
Crooks, Kristy et al. “Cell-free DNA testing in a trisomy 21 pregnancy with confined placental mosaicism for a cell line with trisomy for both chromosomes 18 and 21.” Clinical case reports vol. 4,1 19-22. 9 Nov. 2015, doi:10.1002/ccr3.421.
Join Karyo Club for career insights, case studies, expert-lead discussion and more.